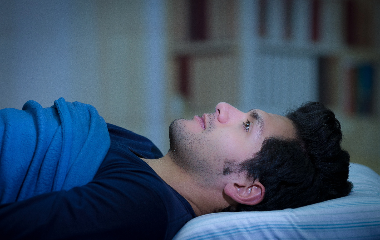
Sleep paralysis is an intriguing and often unnerving phenomenon. Defined as a temporary inability to move or speak while transitioning between sleep and wakefulness, sleep paralysis can be accompanied by vivid hallucinations and a sense of “impending doom.”
Explore the lesser-known aspects of sleep paralysis, including its causes, prevalence, cultural interpretations, and potential remedies.
7 little-known facts about sleep paralysis
1. Sleep paralysis is more common than you might expect.
Research suggests that around 8% of the general population experiences sleep paralysis at some point in their lives. However, certain demographic groups, such as students, people with psychiatric conditions like anxiety or depression, and those with sleep disorders, have a higher likelihood of experiencing sleep paralysis episodes.
2. Different cultures have attempted to explain sleep paralysis through folklore and mythology.
Across the globe, various names and interpretations have emerged, such as the “pisadeira” in Brazil and the “kanashibari” in Japan. In some folklore, sleep paralysis is associated with demons or malevolent spirits that sit on your chest, causing pressure and immobilization. Similarly, stories of alien abductions often parallel the sensations and hallucinations reported during sleep paralysis episodes.
3. You may have vivid hallucinations during sleep paralysis.
One of the most unnerving aspects of sleep paralysis is the presence of vivid and active hallucinations. These hallucinations can take various forms, from dark figures lurking in the room to menacing creatures sitting on your chest. Some researchers believe that these hallucinations stem from the brain’s inability to properly transition between sleep and wakefulness, leading to the blending of dream imagery with the individual’s sense of reality.
4. Several factors can trigger episodes of sleep paralysis.
Sleep deprivation, irregular sleep schedules, and sleep disorders such as narcolepsy have been associated with an increased likelihood of sleep paralysis. In fact, one team of researchers was able to induce episodes of sleep paralysis by depriving participants of REM sleep—a finding that backs up studies pointing to disrupted sleep as a high risk factor. Additionally, stress, anxiety, certain medications, and sleep position have been identified as potential triggers.
5. Sleep paralysis is closely tied to REM sleep.
Normally, your brain prevents your muscles from moving while you’re in REM sleep. It’s a way your brain protects you from acting out your dreams and hurting yourself in your sleep. Sleep paralysis occurs when you regain awareness while you’re either falling asleep or waking up. During sleep paralysis, the vivid dreams of REM sleep can spill over into emerging wakefulness, leading to hallucinations. Research has proposed that overactivation of the amygdala, the brain region responsible for processing emotions and fear, may contribute to the intense feelings of terror experienced during an episode of sleep paralysis.
6. Other sleep disorders may raise the risk of sleep paralysis.
Sleep disorders such as narcolepsy and sleep apnea have been linked to an increased likelihood of experiencing sleep paralysis. Narcolepsy, a neurological disorder characterized by excessive daytime sleepiness and sudden sleep attacks, often involves episodes of sleep paralysis. Sleep apnea, which causes breathing interruptions during sleep, may lead to sleep fragmentation and an increased risk of sleep paralysis.
7. There’s no definitive cure for sleep paralysis.
Treatment of sleep paralysis is aimed at whatever causes it to occur. Several strategies can help manage and reduce its frequency. Because sleep deprivation may trigger sleep paralysis, aim to get 7 or more hours of sleep regularly. Establishing regular sleep patterns, managing stress levels, and improving sleep hygiene can be beneficial. Treating any underlying sleep disorders, such as narcolepsy or sleep apnea, can also help alleviate the recurrence of sleep paralysis symptoms.
Medical review by Rafael Sepulveda-Acosta MD, D-ABOM




{kind=link}
{kind=link}
{kind=link}
{kind=link}